In England and Wales, prison healthcare is supposed to meet the principle of equivalence of care, meaning people in custody should receive the same standard as those in the community. Since 2013, NHS England has commissioned most services on this basis. It is a good promise, but it is not most people’s experience.
Walk onto a prison wing on a weekday morning and you will see the gap between policy and reality. Men queue for their medication, while others panic because their name is not on the list. On the women’s wing, a new mother waits to see a prescriber. None of this is unusual. It is the daily reality of prison healthcare that rationed care long before the public heard the word “backlog”.

The Hidden Barriers to Basic Medication in Prison
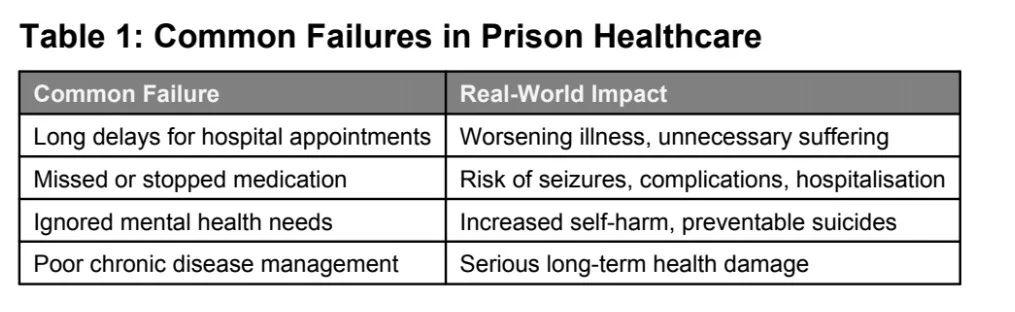
In the community, routine prescriptions are a phone call or an app request. In prison, they are a paperwork relay. You submit a healthcare application, wait for triage, then wait again for a clinic slot. If you need a community-only medicine, it may require an outside appointment that needs an escort. One missed escort can set you back weeks. If there are too few officers to move people, health loses to security. This is a common failure within prison healthcare.
These delays cascade. A diabetic waits for a review to change insulin, an asthmatic runs out of inhalers, and an epileptic struggles to get the timing right when medication rounds are cut short by a lockdown. The Health Services Safety Investigations Body has warned that emergency care in prisons is complicated by the environment. Even calling 999 is slower when a prison is short-staffed or dealing with an incident, another example of the risks around prison healthcare.
People who arrive on remand face a different problem: detox and stabilisation. If the first few days are chaotic, people fall through the gaps. The promise of equivalence becomes a promise to chase, often with a paper slip that disappears under a cell door. This is where prison healthcare often fails to meet its own standards.
The “Escort Economy” and Missed Hospital Appointments
Getting out to hospital is a lottery. Every outside appointment needs two or more officers to escort and supervise a patient. When a prison is short of staff or there is a security incident, healthcare is the first thing to be cancelled. “Security before health” is the unofficial reality. Inspectors have repeatedly found that staffing shortages disrupt access to prison healthcare, including hospital escorts.
For a patient, the cancellation is invisible until the morning you were meant to go. No one calls or emails. You hear at roll-check through a door: “No movement today.”
When that appointment is for a suspected cancer or heart condition, a lost day can turn into months. Prisons and Probation Ombudsman reports are full of cases where repeated cancellations contributed to late diagnosis and avoidable harm. Families often learn this at the inquest, and by then it is a story about a person who should still be alive. These failures sit at the heart of the prison healthcare crisis.

Mental Health: The Longest Queue
If physical healthcare is slow, mental health care is often slower. The demand is higher than in the community, and the environment can make people sicker. When help finally arrives, it is usually a short assessment followed by a long wait for a psychiatrist. The gap between need and provision is one of the starkest features of prison healthcare.
Transfers to secure hospitals can take months while a person deteriorates. Meanwhile, the prison attempts to keep them safe on observation, but this is containment, not treatment. The national data is a stark backdrop, with self-inflicted deaths staying high in recent years.
Medication for mental health has its own hurdles. Many prisons tightly control in-cell possession of psychotropic drugs. This means you may only get your medication when the med round comes by, if the wing is unlocked, if the officer is available, and if the nurse is not pulled to an emergency. These extra steps turn mental health treatment into one of the hardest parts of prison healthcare.
Why This Keeps Happening
- High Demand: People in prison have higher rates of chronic illness, addiction, and severe mental illness than the general population.
- Staffing Shortages: A lack of both clinicians and officers means clinics shrink and escorts vanish, directly limiting prison healthcare.
- Old, Overcrowded Facilities: This makes simple logistics, moving people to healthcare or finding a private room, surprisingly difficult.
- Lack of Transparency: We do not publish comparable data on prison healthcare waiting times the way we do for the community. Without this, a systemic problem is easily dismissed as isolated bad luck.
A Call for Systemic Change
This scandal demands more than quick fixes. We need a plan that:
Publishes the numbers on waiting times and cancellations to hold providers accountable.escorts for urgent cases, fix record-sharing, and measure what matters.
Guarantees escorts for urgent clinical cases.
Creates simple, joined-up digital records that follow a person in real time.
Ensures more prescribers and pharmacists are on site.
Prioritises safe in-cell medication possession.
Provides mental health care that matches the need, with more clinicians and faster transfers.
Uses telemedicine to reduce delays for reviews and follow-ups.
Until then, the advice heard on every wing, “just put in a healthcare slip,” will keep sounding like a shrug from a machine that was never built to say yes.
Equivalence of care is not a luxury. It is the baseline of a civilised system. The law and policy already say it. We do not need new words. We need a plan to move staff into healthcare, ring-fence escorts for urgent cases, fix record-sharing, and measure what matters. Until then, the advice heard on every wing, “just put in a healthcare slip,” will keep sounding like a shrug from a machine that was never built to say yes. Only a serious reform of prison healthcare will change that reality.
If you or a loved one are struggling to access proper prison healthcare, contact Prisoner Rights Legal Services today for advice and support.